Rtms parameters in tinnitus trials: a systematic review
- Select a language for the TTS:
- UK English Female
- UK English Male
- US English Female
- US English Male
- Australian Female
- Australian Male
- Language selected: (auto detect) - EN
Play all audios:

ABSTRACT Over the past few years extensive body of research was produced investigating the effects of repetitive transcranial magnetic stimulation (rTMS) for the treatment of chronic
tinnitus with heterogeneous results. This heterogeneity is exemplified by two recently published large-scale clinical trials reporting different outcomes. Technical aspects of rTMS were
suspected as a potential source for this incongruency. The aim of this systematic review is to examine the overall efficacy as well as to identify possible technical factors relevant for the
effectiveness of rTMS tinnitus trials. Via a literature search appropriate original research papers were identified and rTMS parameters were extracted from each study arm for subsequent
statistical analysis with respect to observed effects (significant vs. not significant pre-post rTMS effects). Our findings indicate that verum rTMS is superior to sham rTMS as demonstrated
by the proportion of significant pre-post contrasts. Some relevant rTMS parameters (e.g., pulse waveform) are not reported. Lower rTMS stimulation intensity was associated with significant
effects in verum rTMS arms. An additional stimulation of the DLPFC to the temporal cortex was not found to promote efficacy. Future research should consider differential effects of rTMS
induced by technical parameters and strive for an exhaustive reporting of relevant rTMS parameters. SIMILAR CONTENT BEING VIEWED BY OTHERS RETROSPECTIVE CHART REVIEW DEMONSTRATING
EFFECTIVENESS OF BIMODAL NEUROMODULATION FOR TINNITUS TREATMENT IN A CLINICAL SETTING Article Open access 28 April 2025 THERAPY EFFECT OF COCHLEURAL ALTERNATING ACOUSTIC BEAM THERAPY VERSUS
TRADITIONAL SOUND THERAPY FOR MANAGING CHRONIC IDIOPATHIC TINNITUS PATIENTS Article Open access 11 March 2024 COMBINING SOUND WITH TONGUE STIMULATION FOR THE TREATMENT OF TINNITUS: A
MULTI-SITE SINGLE-ARM CONTROLLED PIVOTAL TRIAL Article Open access 19 August 2024 INTRODUCTION Chronic subjective tinnitus is defined as the perception of a sound, such as ringing or
buzzing, without the presence of an external or internal source1 with a duration of at least three months2. Approximately 10–15% of people living in industrial countries are affected by such
persistent sounds and up to now, there is no available cure3. Etiology of tinnitus seems to be very heterogeneous, though in most cases it occurs after cochlear damages following noise
trauma or hearing loss in general4. It is assumed, that as a consequence of diminished or missing acoustic input and the ensuing deprivation of neural input in the auditory pathways,
pathological brain changes occur and the “phantom sound”, called tinnitus is generated5,6. From a neurophysiological perspective subjective tinnitus is therefore associated with altered
neural activity along the auditory pathway7 and hyperactivity in auditory brain areas8,9 as well as non-auditory brain areas10. As noted by Theodoroff and Folmer11, these given pathological
neural circumstances represent a significant leverage point for the application of recent neuromodulation techniques, in particular repetitive transcranial magnetic stimulation (rTMS). 15
years ago, low-frequency rTMS of the left auditory cortex was introduced as a new possibility to treat tinnitus based on the rationale to reduce the over-activated left temporal cortex12,13.
Since that time a bulk of trials and also several reviews were published with heterogeneous evaluation of the putative efficacy of rTMS for the treatment of tinnitus. The findings and
conclusions of clinical trials with rTMS in tinnitus manifest to be diverse and are particularly denoted with e.g. high interindividual variability, a lack of sham-controlled trials and
small effect sizes14,15,16. An early review from Langguth _et al_. in 2008 resumed a “promising potential of rTMS for therapeutic management of tinnitus”17. This conclusion is supported by
other reviews, which report rTMS as a new therapeutic tool for tinnitus15, with potential efficacy18, some given evidence19 or even significant medium to large effect sizes as shown by a
meta-analysis20. Furthermore, left temporal low frequency rTMS was declared with a Level C recommendation (possible efficacy) in a consensus statement21. Other reviews indicated “very
limited support for the use of low-frequency rTMS for the treatment of patients with chronic tinnitus”22 or a general tendency to not recommend rTMS for tinnitus23. Beside heterogeneity in
the evaluation of the efficacy of rTMS one aspect past reviews have in common, is a demand for the implementation of randomized, sham-controlled clinical trials with an appropriate sample
size. To the best of our knowledge, two such trials were conducted and published. The ongoing discourse regarding rTMS in tinnitus proceeds by these two clinical trials with an almost
identical methodological design and different reported results. Folmer and colleagues24 were able to show a significant effect of a sham-controlled 1 Hz rTMS protocol over the auditory
cortex on the improvement of tinnitus severity in a study with 64 patients. In contrast, a recent published multi-center study from Landgrebe _et al_.25 involving 146 patients could not
report any improvements as a consequence of rTMS even by investigating a larger sample. It was discussed in subsequent letters to the editors, that differences in samples (e.g., sample
size), used trial design (e.g., outcome measures), but also technical parameters of rTMS (e.g., TMS devices) might be responsible for the conflicting results26,27. In the case of used TMS
devices the direction of current flow differs by default28, which was shown to be critical for the induction of neuroplasticity21,29. Parameter space of technical aspects of rTMS is very
large and all of them seem to be relevant for neurophysiological effects of rTMS30. As early findings indicate and thus as a rule of thumb, low stimulation frequency decreases (≤1 Hz) and
high stimulation frequency increases cortical excitability (≥5 Hz)31,32. In the same manner, the number of pulses delivered per session or the stimulation intensity used, might be essential
for the effectiveness of rTMS33,34. Even if there are plenty of previous reviews, they remain narrow in focus dealing only with effectiveness in general or just patient characteristics, but
do not take the rTMS parameters into account. Hence, the aim of this systematic review is to examine previous research concerning daily rTMS in tinnitus to present a statistical overview of
general effectiveness of rTMS as indicated by verum-sham contrast and to investigate the influence of rTMS parameters on the effect of verum rTMS in tinnitus. MATERIALS AND METHODS PROTOCOL
AND REGISTRATION The review for this paper was conducted according to the guidelines for “Preferred Reporting Items for Systematic Reviews and Meta-Analysis” (PRISMA35; see Supplemental
Material 1). Moreover, the details of the protocol for this review were registered in the International Prospective Register of Systematic Reviews, PROSPERO (CRD42018099744). SEARCH
STRATEGY, STUDY SELECTION AND DATA COLLECTION A systematic literature search was conducted in May 2018 by two independent individuals using the electronic research databases “PubMed” and
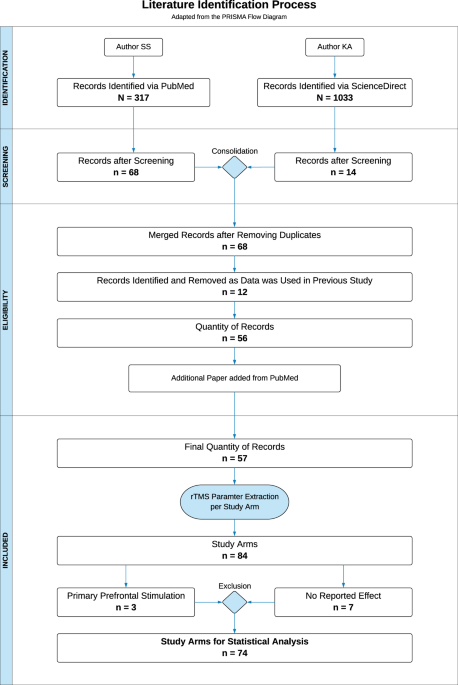
“ScienceDirect” with the keywords “tinnitus” and “transcranial”. Figure 1 provides an overview of the literature identification process by the means of an adapted flow diagram originally
provided by the PRISMA guidelines35. In order to identify a maximum quantity of research papers, the keywords were applied to all possible search fields. The utilization of “PubMed” resulted
in N = 317 potential papers, the search with the database “ScienceDirect” was able to find N = 1.033 articles. An initial screening of the search outcomes was executed by examining the
title as well as the corresponding abstracts with respect to previously defined inclusion criteria: original research data; application of rTMS; repeated sessions; focus on chronic tinnitus.
N = 68 from PubMed and n = 14 from ScienceDirect appropriate research papers could be identified. Hereinafter, the results of both search engines were checked for duplicates and merged to a
consolidated table with n = 68 articles with all publications of the ScienceDirect search included in the PubMed search. In a next step, the papers were resurveyed in full text, to
ascertain, if the studies used data which was already published. As a result, n = 12 papers had to be excluded from our review. Towards the end of the literature identification process, an
additional paper was added as detected by regular PubMed searches. Consequently, the final quantity of records for this review and subsequent analysis consisted of n = 57 research papers. In
order to deploy statistical analysis, important rTMS parameters were extracted from the records for each verum study arm separately. Thus, the parameter extraction of one single paper could
eventuate in multiple study arms for our analysis. Sham arms were not included as we were interested in the effects of rTMS parameters on treatment efficacy. Number of verum and sham arms
were counted for estimation of overall rTMS efficacy (see statistics). Parameters of interest were: manufacturer of the TMS device; type of TMS device; pulse waveform; coil type; coil
orientation; stimulation position; stimulation laterality of auditory cortex stimulation (unilateral or bilateral); unilateral stimulation index (extracted by a calculated ratio for the
stimulated hemisphere (left = 0, right = 1)); the definition of the stimulated hemisphere with respect to tinnitus laterality; stimulation frequency (Hz) (condensed to inhibitory or
excitatory frequency protocols for analysis); stimulation intensity (% of motor threshold); mean motor threshold (%); motor threshold determination method (electromyography (EMG)/visual);
number of sessions; overall pulses per session over auditory and prefrontal cortical areas; pulses per session over auditory cortical areas; overall total pulses over auditory and prefrontal
cortical areas (calculated as the number of pulses per session * number of sessions); total pulses over auditory cortical (defined as the number of auditory pulses per session * number of
sessions); use of a neuronavigation system (yes/no); additional stimulation (e.g., frontal stimulation additionally to auditory cortex stimulation; stimulation parameters were extracted
equally; cf. Supplemental Material 2). Further study-specific information like type of additional treatment, study design or used outcome measurements were also extracted from the records,
simply to provide an overview and were not considered for statistical analysis. As no study arm reported the used pulse waveform, we decided to perform statistical analysis for this purpose
with the default waveform of the used TMS devices. The information was gathered from user manuals and by contacting the manufacturers of the devices or the authors of the papers,
respectively. Our dependent variable of interest was the reported effect of each of the study arms dichotomized to “significant” and “not significant”, as most papers did not report effect
sizes. Since only N = 38 study arms provided information about the definition of a primary outcome instrument, a study arm was declared as significant, if 50% or more of the used outcome
measurements were reported as “significant”. In case of a lack of information concerning relevant parameters or outcomes, the term “not reported” was used and was not considered in the
definition of the reported effect. DATA ANALYSIS Statistical analysis was performed with the statistic software R (R version 3.4.3; R Foundation for Statistical Computing, Austria; packages
“tidyverse and “gmodels”) and focused on the change of symptoms from pre to post treatment of each extracted study arm. For all analyses, we concentrated on trials using stimulation of the
temporal or temporoparietal cortex as most studies primarily stimulated these areas (for details see results section) and thus stimulation positions restricted solely to areas outside the
temporal region were excluded (three study arms including prefrontal cortex). For seven study arms no information was provided about whether pre to post rTMS changes were significant or not.
Therefore, n = 10 study arms were excluded, resulting in 74 study arms included in statistical analyses (cf. Fig. 1). Missing values, “not-reported” effects or information only provided in
certain ranges (e.g., pulses per session 1800–3000) were excluded for each parameter analysis individually. Parameters were not analyzed, if 30% of the investigated arms did not provide
data. Associations of categorical data with the reported effects (significant vs. not significant) were calculated with χ2-tests and Fisher’s exact tests in the case of cell frequencies
below 5. To evaluate differences in parametric variables regarding the given effect, Mann-Whitney U-tests for independent samples were computed. Significance level was defined as p ≤ 0.05
and reported uncorrected for multiple comparisons. RESULTS The extraction of relevant parameters from N = 57 research papers resulted in overall N = 74 study arms for which statistical
comparisons from pre to post rTMS treatment were done. A detailed overview of the descriptive statistics of rTMS parameters of the single study arms can be found in Supplemental Material 2.
Out of 74 study arms used for statistics, 56 arms reported significant effects (76%). In order to ascertain whether the efficacy of verum rTMS is higher in contrast to sham rTMS, we
statistically compared the quantity of reported significant and not significant results of verum study arms with those of available 22 sham arms (5 significant; 23%). A χ2-test indicated a
significant association of the type of study arm (verum or sham) and rTMS efficacy (pre-post change significant or not) showing a superiority of verum in contrast to sham rTMS (p < 0.05).
Table 1 shows the results of the association of technical rTMS parameters with efficacy as indicated by pre-post changes in verum study arms. Analyses of parametric data revealed that the
group of significant study arms, showed lower stimulation intensity (about 6.5% stimulator output) in contrast to not significant arms (cf. Fig. 2). Out of 18 study arms utilizing a
stimulation intensity lower than 110%, 94.44% reported significant results. Whereas, in case of ≥110% stimulation intensity (two study arms with 120% stimulation intensity; one significant,
one not significant), 68.00% of 50 study arms state significant findings.” To exclude a potential confounder caused by studies applying continuous theta burst stimulation (cTBS) using
commonly lower stimulation intensities, we investigated a possible association of cTBS or rTMS with reported effects. Our results show no significant association (proportion of significant
studies did not differ between cTBS and rTMS studies; cf. Table 1), indicating an exclusion of this potential bias in our stimulation intensity results. With respect to number of pulses,
significant study arms used less pulses. Since the number of pulses was only significant for overall pulses per session, we compared the reported effects of study arms which used an
additional DLPFC stimulation (n = 16) with those free of any additional stimulation, as DLPFC stimulation in addition to auditory cortex stimulation might result more applied pulses. Indeed,
a significant difference was found in the used number of pulses between arms with additional prefrontal stimulation (3056.25 ± 871.78) and those with only temporal rTMS (1672.28 ± 723.44),
U = 108.50, p < 0.01. As pointed out in Table 1, a _χ_2-test found a significant association between the use of an additional DLPFC stimulation and whether or not the effect of rTMS was
significant. Since 80.70% of the study arms without an additional stimulation of the DLPFC report significant results, whereas only 56.25% of the study arms with an additional stimulation
show significant effects, our findings suggest no benefit of an additional DLPFC stimulation, rather the opposite seems to pertain. In order to preclude a potential publication bias caused
by a possible high quantity of significant or not significant results published in certain years (e.g., more significant studies in early years and more not significant studies in late
years36), publication years of 57 study arms with solely auditory cortex rTMS were considered for statistical analysis to check if there is a mean difference between significant and not
significant effects. No significant difference was found, perpending an exclusion of a publication bias, U = 241.50, p = 0.82. Figure 3 presents a summary of the quantity of published
auditory cortex rTMS trial arms for each year subdivided by the reported effect. All other parametric parameters were not significant. Mean motor threshold was not analyzed due to more than
30% of missing data (n = 65). Analysis of categorical data showed no significant associations e.g. between the manufacturer of the TMS device (Magstim vs. MagVenture/Medtronic; number of
other manufacturers were too low to include in analysis) or the default waveform of the system (biphasic cosine vs. biphasic sine). Coil orientation was not analyzed, because it was not
reported in 34 study arms. Likewise, the type of coil was not included in statistical analysis, since 93.2% of examined arms used a figure-of-eight coil. Table 2 provides an overview over
the missing information for all parameters separated for significant and not significant study arms. DISCUSSION Due to ongoing discussions about the effectiveness of rTMS in chronic tinnitus
and recently initiated considerations if beside methodological also technical parameters of rTMS affect treatment efficacy, we conducted a systematic review of previous research concerning
daily rTMS in tinnitus with the aim to present a statistical overview of general effectiveness of rTMS and to identify the influence of rTMS parameters on the consequences of verum rTMS in
tinnitus. With respect to the question if rTMS is generally effective as a treatment in tinnitus, we demonstrated that the proportion of significant pre-post comparisons is significantly
higher for verum in contrast to sham arms. The chosen statistical strategy with observed effects dichotomized to “significant” and “not significant” is limited. Meta-analyses are rather
suitable as a statistical approach to resolve this question. Furthermore, the quantity of eligible studies might be too low for valid analysis at this stage. Despite two recently published
large trials with contradictory findings24,25, the debate on recommendation of auditory cortex rTMS for the treatment of chronic tinnitus is still not completed. We explored two main
associations of technical parameters on rTMS efficacy. First, we found that a lower stimulation intensity was associated with significance in the investigated study arms. This finding is in
contrast to earlier work in depression and basic research concerning the motor cortex, which suggested a linear dose-response relationship, e.g. better treatment response34,37 or an
increased influence on motor evoked potentials (MEPs)33,38 is associated with higher stimulation intensity. A clarification of the detected reversed impact appears to be difficult. One
feasible explanation for this could be, that the stimulation intensity generates the intended consequences only up to a certain extent and then the effect either disappears or inverts.
Similar changes are observed by the use of cTBS, which is also known to generate inhibitory effects such as 1 Hz rTMS. Applied at higher stimulation intensities, the inhibitory effects shift
to excitatory39,40. These observations somewhat corroborate our findings, although with our collected data and statistical analysis we are not able to make a statement about possible
excitatory effects of high stimulation intensities. A further possible explanation could be related to skull thickness. Compared to the rest of the cranium, the average bone thickness over
temporal parts is described as the thinnest41. Due to the location of the primary motor cortex under thicker bones, namely the interface of the frontal and parietal osseous, the motor
threshold at this position might be an insufficient point of reference for the determination of the stimulation intensity for other stimulation positions. With respect to our results, a high
intensity rTMS over thinner temporal bones might result in some kind of hyperstimulation which may induce contrary effects as argued above. Higher stimulation intensity potentially caused
by visual determination of the motor threshold42 as well as a lower intensities caused by cTBS were excluded as shown by our analysis (cf. results section). Secondly, the present systematic
review indicates, that the lower number of pulses, including auditory and prefrontal cortical areas (per session and also for the whole trial), the more significant study arms were found.
With regard to TBS, past research already investigated the effects of longer stimulation protocols with the insight that a prolongation of the stimulation per se does not lead to an
improvement. A doubling of the stimulation length induced reversed after-effects e.g. inhibitory became excitatory43. For rTMS, a meta-analysis reported similar results, indicating a smaller
number of pulses per session related to antidepressant mechanism of action44. The authors of this meta-analysis refer to other conducted meta-analyses with no such association – the key
role of the quantity of pulses remains to be clarified. The same applies for the field of tinnitus. Former studies observed a substantial improvement in tinnitus-related outcome measurements
with the usage of a higher number of pulses45,46. In contrast our investigation suggests the complete opposite. It is very probable, that the effect is conceivably caused by an additional
stimulation of the DLPFC, which features significant more pulses per session (cf. results section). Based on the rationale that via prefrontal rTMS anti-depressant effects take place21, an
assumed interplay of tinnitus and depression47,48 and the involvement of prefrontal areas in auditory gating and tinnitus, combined frontal and temporal rTMS was proposed for more efficient
suppression of tinnitus symptoms49,50,51. In contrast, our results are not in accordance with these findings. Addition of prefrontal rTMS eventuated in a significantly lower percentage of
significant effects. In tinnitus, not only prefrontal areas, rather several cortical regions are involved, suggesting a widely spread network and also interindividual network
profiles52,53,54,55. This postulation of several involved regions offers a putative approach to explain the unfavorable effect of additional prefrontal rTMS as only a “prefrontal” subtype
would best benefit from this treatment and in other subtypes it might be contraindicative. Our finding of better effects of merely temporal stimulation provides support for the notion, that
the final common pathway of tinnitus related pathophysiological alterations might still be the auditory cortex56. One might argue that initial positive findings of solely auditory cortex
stimulation motivated the field to concentrate on this stimulation protocol and might have induced a publication bias in the sense that initial clinical trials are often reported as
promising with large effect sizes followed by years of increasing frustration showing a decrease of effect sizes and an increase of negative trials. Our analysis indicates that there is no
change in the number of significant studies published per year (see Fig. 3) not revealing a potential publication bias with a time trend. Due to the limited amount of data we were only able
to analyze the effects of single rTMS parameters alone. However, we are aware of the possibility of specific interactions of several parameters, as demonstrated by pulse-quantity-dependent
after-effects of excitatory intermittent theta burst stimulation (iTBS) on MEPS to be more distinct after lower stimulation intensities57. Likewise, it may be possible, that the inequality
in the number of significant (n = 56) and not significant (n = 18) study arms bears an influence on our results. Howsoever, the role of stimulation intensities and pulses per session for the
effectiveness of rTMS needs to be systematically examined to clarify the outstanding issues of dose-dependent effects in tinnitus trials, especially as these findings are contradictory to
the experiences of rTMS for the treatment of depression58. One of the initial intentions of this review was to investigate the effect of different waveforms on the effectiveness of rTMS.
Unfortunately, not a single study reported the used pulse waveform for the stimulation. We have therefore decided to statistically analyze the default waveform settings of the device. We
found no significant association between the type of biphasic waveform and the significance level of the effect. It was stated, that the coil orientation and the related induced direction of
the currents are crucial in rTMS59,60,61. Biphasic pulses appear to be stronger, when passing the area of interest in anterior-posterior direction28. Due to many missing in the reported
data, it was not possible to analyze the critical parameter current direction. With the emerge of new technical innovations in the field of brain stimulation, exact stimulation positions via
TMS integrated neuronavigation systems became a standard procedure. This review intended to determine the benefits of TMS neuronavigation systems in tinnitus. No such benefit is implied by
our results. Either the local precision of stimulation does not play such a big role as presumed, or the targets were not optimally selected. Technical parameters like intensity or pulses,
with neural mechanism not entirely understood, seem to be more important. Several considerable methodological disadvantages were observed in the course of this review. A very important
parameter in order to compare outcomes of different studies and even specify the effectiveness of a specific intervention is the definition of a primary outcome. We identified a lack of this
information in N = 36 study arms of interest, leading to an adapted definition of observed significance for our review. In the course of examining appropriate research papers, unexpected
differences (e.g., breaks during stimulation) within the methodology of 1 Hz rTMS were observed in some of the studies62,63,64,65,66,67. Such conditions make a comparison of trials even more
difficult and introduce noise to the data. A major insight of the present work is the lack of reported essential rTMS parameters in the literature. Not only the full information about the
used waveform was missing, but also relevant data on coil orientation or mean motor threshold features many missing values (cf. Table 2), which restricted our analysis. Guidelines for
reporting e.g. the interventional methods used in clinical trials68 or a checklist for reporting parameters when deploying TMS on the motor system69 already exist. A paper from Wilson &
St George70 and a recent review focusing on rTMS in the context of depression71 already emphasize the need of fully reported methodological information. The latter even provides a checklist
for reporting rTMS parameters. Since both checklists enumerate essential parameters and details for rTMS, we strongly recommend their usage in future studies, to prospectively ensure a more
precise and fundamental comparison of non-invasive brain stimulation studies using rTMS. CONCLUSION The present systematic review demonstrates a higher efficacy of verum rTMS in contrast to
sham rTMS. In verum arms, technical parameters such as stimulation intensity and number of pulses or restrictive stimulation of the auditory cortex were identified as relevant factors for
clinical efficacy in a dose-dependent manner – less might be more. The impact of technical parameters in interaction with neurophysiological parameters (e.g., brain state before
stimulation72,73,74) highlights the capability of rTMS in treating chronic tinnitus based on the premise to identify optimal stimulation protocols for single patients by means of
personalized medical approaches75. In order to understand the consequences of considerable rTMS parameters in detail, standardized and sufficient reporting is highly required. As of yet,
this is not the case – neither in tinnitus research nor in any other field utilizing
rTMS24,25,45,49,50,51,62,63,64,65,66,67,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119.
REFERENCES * Erlandsson, S. & Dauman, N. Categorization of tinnitus in view of history and medical discourse. _Int. J. Qual. Stud. Health Well-Being_ 8, 23530 (2013). Article PubMed
Google Scholar * Hall, D. A. Treatment options for subjective tinnitus: Self reports from a sample of general practitioners and ENT physicians within Europe and the USA. 15 (2011). *
Heller, A. J. Classification and epidemiology of tinnitus. _Otolaryngol. Clin. North Am._ 36, 239–248 (2003). Article PubMed Google Scholar * Langguth, B., Kreuzer, P. M., Kleinjung, T.
& De Ridder, D. Tinnitus: causes and clinical management. _Lancet Neurol._ 12, 920–930 (2013). Article PubMed Google Scholar * Eggermont, J. J. Pathophysiology of tinnitus. _Prog.
Brain Res._ 166, 19–35 (2007). Article CAS PubMed Google Scholar * Eggermont, J. J. & Tass, P. A. Maladaptive Neural Synchrony in Tinnitus: Origin and Restoration. _Front. Neurol_. 6
(2015). * Eggermont, J. J. & Roberts, L. E. The Neuroscience of Tinnitus: Understanding Abnormal and Normal Auditory Perception. _Front. Syst. Neurosci_. 6 (2012). * Farhadi, M. _et
al_. Functional brain abnormalities localized in 55 chronic tinnitus patients: fusion of SPECT coincidence imaging and MRI. _J. Cereb. Blood Flow Metab. Off. J. Int. Soc. Cereb. Blood Flow
Metab._ 30, 864–870 (2010). Article Google Scholar * Folmer, R. L. Lateralization of neural activity associated with tinnitus. _Neuroradiology_ 49, 689–691; author reply 693–696 (2007).
Article ADS PubMed Google Scholar * Vanneste, S. & De Ridder, D. The auditory and non-auditory brain areas involved in tinnitus. An emergent property of multiple parallel overlapping
subnetworks. _Front. Syst. Neurosci._ 6, 31 (2012). Article PubMed PubMed Central Google Scholar * Theodoroff, S. M. & Folmer, R. L. Repetitive Transcranial Magnetic Stimulation as
a Treatment for Chronic Tinnitus. _A Critical Review._ 34, 10 (2013). Google Scholar * Eichhammer, P., Langguth, B., Marienhagen, J., Kleinjung, T. & Hajak, G. Neuronavigated repetitive
transcranial magnetic stimulation in patients with tinnitus: a short case series. _Biol. Psychiatry_ 54, 862–865 (2003). Article PubMed Google Scholar * Langguth, B. _et al_.
Neuronavigated rTMS in a patient with chronic tinnitus. Effects of 4 weeks treatment. _Neuroreport_ 14, 977–980 (2003). Article PubMed Google Scholar * Langguth, B. & De Ridder, D.
Tinnitus: therapeutic use of superficial brain stimulation. _Handb. Clin. Neurol._ 116, 441–467 (2013). Article PubMed Google Scholar * Peng, Z., Chen, X.-Q. & Gong, S.-S.
Effectiveness of Repetitive Transcranial Magnetic Stimulation for Chronic Tinnitus: A Systematic Review. _Otolaryngol.-Head Neck Surg._ 147, 817–825 (2012). Article PubMed Google Scholar
* Plewnia, C. Brain Stimulation: New Vistas for the Exploration and Treatment of Tinnitus: Brain Stimulation. _CNS Neurosci. Ther._ 17, 449–461 (2011). Article PubMed Google Scholar *
Langguth, B. _et al_. Controversy: Does repetitive transcranial magnetic stimulation/transcranial direct current stimulation show efficacy in treating tinnitus patients? _Brain Stimulat._ 1,
192–205 (2008). Article Google Scholar * Londero, A., Bonfils, P. & Lefaucheur, J. P. Transcranial magnetic stimulation and subjective tinnitus. A review of the literature, 2014–2016.
_Eur. Ann. Otorhinolaryngol. Head Neck Dis._ 135, 51–58 (2018). Article CAS PubMed Google Scholar * Donaldson, P. H., Rinehart, N. J. & Enticott, P. G. Noninvasive stimulation of
the temporoparietal junction: A systematic review. _Neurosci. Biobehav. Rev._ 55, 547–572 (2015). Article PubMed Google Scholar * Soleimani, R., Jalali, M. M. & Hasandokht, T.
Therapeutic impact of repetitive transcranial magnetic stimulation (rTMS) on tinnitus: a systematic review and meta-analysis. _Eur. Arch. Otorhinolaryngol._ 273, 1663–1675 (2016). Article
PubMed Google Scholar * Lefaucheur, J.-P. _et al_. Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS). _Clin. Neurophysiol._ 125,
2150–2206 (2014). Article PubMed Google Scholar * Meng, Z., Liu, S., Zheng, Y. & Phillips, J. S. Repetitive transcranial magnetic stimulation for tinnitus. _Cochrane Database Syst.
Rev._ https://doi.org/10.1002/14651858.CD007946.pub2 (2011). Article PubMed Google Scholar * Zenner, H.-P. _et al_. A multidisciplinary systematic review of the treatment for chronic
idiopathic tinnitus. _Eur. Arch. Otorhinolaryngol._ 274, 2079–2091 (2017). Article PubMed Google Scholar * Folmer, R. L. _et al_. Repetitive Transcranial Magnetic Stimulation Treatment
for Chronic Tinnitus: A Randomized Clinical Trial. _JAMA Otolaryngol.–Head Neck Surg._ 141, 716–722 (2015). Article PubMed CAS Google Scholar * Landgrebe, M. _et al_. 1-Hz rTMS in the
treatment of tinnitus: A sham-controlled, randomized multicenter trial. _Brain Stimulat._ 10, 1112–1120 (2017). Article Google Scholar * Folmer, R. L. Factors that contribute to the
efficacy of repetitive transcranial magnetic stimulation (rTMS) for tinnitus treatment. _Brain Stimulat._ 10, 1121–1122 (2017). Article Google Scholar * Landgrebe, M., Schecklmann, M.
& Langguth, B. Reply to the letter of Robert L. Folmer: Does treatment response depend on the type of stimulation device? _Brain Stimulat._ 10, 1123–1124 (2017). Article Google Scholar
* Kammer, T., Beck, S., Thielscher, A., Laubis-Herrmann, U. & Topka, H. Motor thresholds in humans: a transcranial magnetic stimulation study comparing different pulse waveforms,
current directions and stimulator types. _Clin. Neurophysiol._ 112, 250–258 (2001). Article CAS PubMed Google Scholar * Sommer, M. & Paulus, W. TMS waveform and current direction.
_Oxf. Handb. Transcranial Stimul._ https://doi.org/10.1093/oxfordhb/9780198568926.013.0002 (2008). Article Google Scholar * Rossini, P. M. _et al_. Non-invasive electrical and magnetic
stimulation of the brain, spinal cord, roots and peripheral nerves: Basic principles and procedures for routine clinical and research application. An updated report from an I.F.C.N.
Committee. _Clin. Neurophysiol. Off. J. Int. Fed. Clin. Neurophysiol._ 126, 1071–1107 (2015). Article CAS Google Scholar * Hoffman, R. E. & Cavus, I. Slow transcranial magnetic
stimulation, long-term depotentiation, and brain hyperexcitability disorders. _Am. J. Psychiatry_ 159, 1093–1102 (2002). Article PubMed Google Scholar * Pascual-Leone, A., Valls-Solé, J.,
Wassermann, E. M. & Hallett, M. Responses to rapid-rate transcranial magnetic stimulation of the human motor cortex. _Brain J. Neurol._ 117(Pt 4), 847–858 (1994). Article Google
Scholar * Fitzgerald, P. Intensity-dependent effects of 1 Hz rTMS on human corticospinal excitability. _Clin. Neurophysiol._ 113, 1136–1141 (2002). Article PubMed Google Scholar *
Padberg, F. _et al_. Repetitive Transcranial Magnetic Stimulation (rTMS) in Major Depression: Relation between Efficacy and Stimulation Intensity. _Neuropsychopharmacology_ 27, 638–645
(2002). Article PubMed Google Scholar * Moher, D., Liberati, A., Tetzlaff, J. & Altman, D. G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement.
_PLoS Med._ 6, 6 (2009). Article Google Scholar * Jennions, M. D. & Møller, A. P. Relationships fade with time: a meta-analysis of temporal trends in publication in ecology and
evolution. _Proc. R. Soc. B Biol. Sci._ 269, 43–48 (2002). Article Google Scholar * Fitzgerald, P. B., Hoy, K. E., Anderson, R. J. & Daskalakis, Z. J. A study of the pattern of
response to Rtms treatment in depression. _Depress. Anxiety_ 33, 746–753 (2016). Article PubMed Google Scholar * Lang, N. _et al_. Stimulus intensity and coil characteristics influence
the efficacy of rTMS to suppress cortical excitability. _Clin. Neurophysiol._ 117, 2292–2301 (2006). Article PubMed Google Scholar * Sasaki, T. _et al_. The intensity of continuous theta
burst stimulation, but not the waveform used to elicit motor evoked potentials, influences its outcome in the human motor cortex. _Brain Stimul. Basic Transl. Clin. Res. Neuromodulation_ 11,
400–410 (2018). Google Scholar * Gentner, R., Wankerl, K., Reinsberger, C., Zeller, D. & Classen, J. Depression of Human Corticospinal Excitability Induced by Magnetic Theta-burst
Stimulation: Evidence of Rapid Polarity-Reversing Metaplasticity. _Cereb. Cortex_ 18, 2046–2053 (2008). Article PubMed Google Scholar * Mahinda, H. A. M. & Murty, O. P. Variability in
thickness of human skull bones and sternum – an autopsy experience. _J. Forensic Med._ 26, 7 (2009). Google Scholar * Westin, G. G., Bassi, B. D., Lisanby, S. H. & Luber, B.
Determination of motor threshold using visual observation overestimates transcranial magnetic stimulation dosage: Safety implications. _Clin. Neurophysiol. Off. J. Int. Fed. Clin.
Neurophysiol._ 125, 142–147 (2014). Article Google Scholar * Gamboa, O. L., Antal, A., Moliadze, V. & Paulus, W. Simply longer is not better: reversal of theta burst after-effect with
prolonged stimulation. _Exp. Brain Res. Exp. Hirnforsch. Exp. Cerebrale_ 204, 181–187 (2010). Article Google Scholar * Kedzior, Azorina, V. & Reitz, S. More female patients and fewer
stimuli per session are associated with the short-term antidepressant properties of repetitive transcranial magnetic stimulation (rTMS): a meta-analysis of 54 sham-controlled studies
published between 1997–2013. _Neuropsychiatr. Dis. Treat_. 727, https://doi.org/10.2147/NDT.S58405 (2014). * Park, J. H. _et al_. Difference in Tinnitus Treatment Outcome According
to the Pulse Number of Repetitive Transcranial Magnetic Stimulation. _Otol. Neurotol. Off. Publ. Am. Otol. Soc. Am. Neurotol. Soc. Eur. Acad. Otol. Neurotol._ 36, 1450–1456 (2015). Article
Google Scholar * Plewnia, C. _et al_. Dose-dependent attenuation of auditory phantom perception (tinnitus) by PET-guided repetitive transcranial magnetic stimulation. _Hum. Brain Mapp._
28, 238–246 (2007). Article PubMed Google Scholar * Geocze, L., Mucci, S., Abranches, D. C., Marco, M. A. & Penido, N. O. Systematic review on the evidences of an association between
tinnitus and depression. _Braz. J. Otorhinolaryngol._ 79, 106–111 (2013). Article PubMed Google Scholar * Ziai, K., Moshtaghi, O., Mahboubi, H. & Djalilian, H. R. Tinnitus Patients
Suffering from Anxiety and Depression: A Review. _Int. Tinnitus J._ 21, 68–73 (2017). Article PubMed Google Scholar * Kleinjung, T. _et al_. Combined temporal and prefrontal transcranial
magnetic stimulation for tinnitus treatment: a pilot study. _Otolaryngol.–Head Neck Surg. Off. J. Am. Acad. Otolaryngol.-Head Neck Surg._ 138, 497–501 (2008). Article Google Scholar *
Langguth, B. _et al_. Efficacy of different protocols of transcranial magnetic stimulation for the treatment of tinnitus: Pooled analysis of two randomized controlled studies. _World J.
Biol. Psychiatry Off. J. World Fed. Soc. Biol. Psychiatry_ 15, 276–285 (2014). Article CAS Google Scholar * Lehner, A. _et al_. Multisite rTMS for the treatment of chronic tinnitus:
stimulation of the cortical tinnitus network–a pilot study. _Brain Topogr._ 26, 501–510 (2013). Article PubMed Google Scholar * Adjamian, P., Sereda, M. & Hall, D. A. The mechanisms
of tinnitus: Perspectives from human functional neuroimaging. _Hear. Res._ 253, 15–31 (2009). Article PubMed Google Scholar * Elgoyhen, A. B., Langguth, B., De Ridder, D. & Vanneste,
S. Tinnitus: perspectives from human neuroimaging. _Nat. Rev. Neurosci._ 16, 632–642 (2015). Article CAS PubMed Google Scholar * Lanting, C. P., de Kleine, E. & van Dijk, P. Neural
activity underlying tinnitus generation: results from PET and fMRI. _Hear. Res._ 255, 1–13 (2009). Article CAS PubMed Google Scholar * Schlee, W. _et al_. Mapping cortical hubs in
tinnitus. _BMC Biol._ 7, 80 (2009). Article PubMed PubMed Central Google Scholar * Schecklmann, M. _et al_. Auditory cortex is implicated in tinnitus distress: a voxel-based morphometry
study. _Brain Struct. Funct._ 218, 1061–1070 (2013). Article CAS PubMed Google Scholar * Nettekoven, C. _et al_. Dose-dependent effects of theta burst rTMS on cortical excitability and
resting-state connectivity of the human motor system. _J. Neurosci. Off. J. Soc. Neurosci._ 34, 6849–6859 (2014). Article CAS Google Scholar * Gershon, A. A., Dannon, P. N. &
Grunhaus, L. Transcranial magnetic stimulation in the treatment of depression. _Am. J. Psychiatry_ 160, 835–845 (2003). Article PubMed Google Scholar * Kammer, T., Beck, S., Erb, M. &
Grodd, W. The influence of current direction on phosphene thresholds evoked by transcranial magnetic stimulation. _Clin. Neurophysiol._ 112, 2015–2021 (2001). Article CAS PubMed Google
Scholar * Mills, K. R., Boniface, S. J. & Schubert, M. Magnetic brain stimulation with a double coil: the importance of coil orientation. _Electroencephalogr. Clin. Neurophysiol.
Potentials Sect._ 85, 17–21 (1992). Article CAS Google Scholar * Sale, M. V., Lavender, A. P., Opie, G. M., Nordstrom, M. A. & Semmler, J. G. Increased intracortical inhibition in
elderly adults with anterior–posterior current flow: A TMS study. _Clin. Neurophysiol._ 127, 635–640 (2016). Article PubMed Google Scholar * Kim, B. G. _et al_. Comparison of the outcomes
of repetitive transcranial magnetic stimulation to the ipsilateral and contralateral auditory cortex in unilateral tinnitus. _Electromagn. Biol. Med._ 33, 211–215 (2014). Article PubMed
Google Scholar * Kim, H. J. _et al_. Long-term effects of repetitive transcranial magnetic stimulation in unilateral tinnitus. _The Laryngoscope_ 124, 2155–2160 (2014). Article PubMed
Google Scholar * Piccirillo, J. F. _et al_. Low-frequency repetitive transcranial magnetic stimulation to the temporoparietal junction for tinnitus. _Arch. Otolaryngol. Head Neck Surg._
137, 221–228 (2011). Article PubMed PubMed Central Google Scholar * Piccirillo, J. F. _et al_. Low-frequency repetitive transcranial magnetic stimulation to the temporoparietal junction
for tinnitus: four-week stimulation trial. _JAMA Otolaryngol.–Head Neck Surg._ 139, 388–395 (2013). Article PubMed PubMed Central Google Scholar * Rossi, S. _et al_. Effects of
repetitive transcranial magnetic stimulation on chronic tinnitus: a randomised, crossover, double blind, placebo controlled study. _J. Neurol. Neurosurg. Psychiatry_ 78, 857–863 (2007).
Article ADS PubMed PubMed Central Google Scholar * Yang, H. _et al_. The Characteristic and Changes of the Event-Related Potentials (ERP) and Brain Topographic Maps before and after
Treatment with rTMS in Subjective Tinnitus Patients. _PLoS ONE_ 8, e70831 (2013). Article ADS CAS PubMed PubMed Central Google Scholar * Schulz, K. F., Altman, D. G. & Moher, D.
CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. _J. Pharmacol. Pharmacother._ 1, 100–107 (2010). Article PubMed PubMed Central Google Scholar *
Chipchase, L. _et al_. A checklist for assessing the methodological quality of studies using transcranial magnetic stimulation to study the motor system: An international consensus study.
_Clin. Neurophysiol._ 123, 1698–1704 (2012). Article PubMed PubMed Central Google Scholar * Wilson, M. T. & St George, L. Repetitive Transcranial Magnetic Stimulation: A Call for
Better Data. _Front. Neural Circuits_ 10 (2016). * Chantebel, R., Chesneau, A., Tavernier, E., El-Hage, W. & Caille, A. Completeness of Descriptions of Repetitive Transcranial Magnetic
Stimulation Intervention: A Systematic Review of Randomized Controlled Trials of rTMS in Depression. _J. ECT_, https://doi.org/10.1097/YCT.0000000000000546 (2018). Article PubMed Google
Scholar * Weisz, N., Steidle, L. & Lorenz, I. Formerly known as inhibitory: effects of 1-Hz rTMS on auditory cortex are state-dependent: Formerly known as inhibitory. _Eur. J.
Neurosci._ 36, 2077–2087 (2012). Article PubMed Google Scholar * Siebner, H. R. _et al_. Preconditioning of low-frequency repetitive transcranial magnetic stimulation with transcranial
direct current stimulation: evidence for homeostatic plasticity in the human motor cortex. _J. Neurosci. Off. J. Soc. Neurosci._ 24, 3379–3385 (2004). Article CAS Google Scholar *
Silvanto, J. & Pascual-Leone, A. State-Dependency of Transcranial Magnetic Stimulation. _Brain Topogr._ 21, 1–10 (2008). Article PubMed PubMed Central Google Scholar * Kreuzer, P. M.
_et al_. Combined rTMS treatment targeting the Anterior Cingulate and the Temporal Cortex for the Treatment of Chronic Tinnitus. _Sci. Rep._ 5, 18028 (2015). Article ADS CAS PubMed
PubMed Central Google Scholar * Vielsmeier, V. _et al_. A Pilot Study of Peripheral Muscle Magnetic Stimulation as Add-on Treatment to Repetitive Transcranial Magnetic Stimulation in
Chronic Tinnitus. _Front. Neurosci._ 12, 68 (2018). Article PubMed PubMed Central Google Scholar * Cacace, A. T. _et al_. Glutamate is down-regulated and tinnitus loudness-levels
decreased following rTMS over auditory cortex of the left hemisphere: A prospective randomized single-blinded sham-controlled cross-over study. _Hear. Res._
https://doi.org/10.1016/j.heares.2017.10.017 (2017). Article PubMed Google Scholar * James, G. A. _et al_. Neural activity during attentional conflict predicts reduction in tinnitus
perception following rTMS. _Brain Stimulat._ 10, 934–943 (2017). Article CAS Google Scholar * Noh, T.-S. _et al_. Comparison of treatment outcomes between 10 and 20 EEG electrode location
system-guided and neuronavigation-guided repetitive transcranial magnetic stimulation in chronic tinnitus patients and target localization in the Asian brain. _Acta Otolaryngol. (Stockh.)_
137, 945–951 (2017). Article Google Scholar * Kreuzer, P. M. _et al_. Individualized Repetitive Transcranial Magnetic Stimulation Treatment in Chronic Tinnitus? _Front. Neurol._ 8, 126
(2017). Article PubMed PubMed Central Google Scholar * Noh, T.-S. _et al_. Comparison of Treatment Outcomes Following Either Prefrontal Cortical-only or Dual-site Repetitive Transcranial
Magnetic Stimulation in Chronic Tinnitus Patients: A Double-blind Randomized Study. _Otol. Neurotol. Off. Publ. Am. Otol. Soc. Am. Neurotol. Soc. Eur. Acad. Otol. Neurotol._ 38, 296–303
(2017). Article Google Scholar * Wang, H. _et al_. Factor Analysis of Low-Frequency Repetitive Transcranial Magnetic Stimulation to the Temporoparietal Junction for Tinnitus. _Neural
Plast._ 2016, 2814056 (2016). PubMed PubMed Central Google Scholar * Labar, D., Labar, A. S. & Edwards, D. Long-Term Distributed Repetitive Transcranial Magnetic Stimulation for
Tinnitus: A Feasibility Study. _Neuromodulation J. Int. Neuromodulation Soc._ 19, 249–253 (2016). Article Google Scholar * Wang, H., Li, B., Wu, H., Shi, H. & Yin, S. Combination of
gaps in noise detection and visual analog scale for measuring tinnitus components in patients treated with repetitive transcranial magnetic stimulation. _Auris. Nasus. Larynx_ 43, 254–258
(2016). Article CAS PubMed Google Scholar * Lo, Y. L. _et al_. A comparison study of repetitive transcranial magnetic stimulation for tinnitus treatment in an Asian population. _Clin.
Neurol. Neurosurg._ 119, 96–99 (2014). Article CAS PubMed Google Scholar * Bilici, S., Yigit, O., Taskin, U., Gor, A. P. & Yilmaz, E. D. Medium-term results of combined treatment
with transcranial magnetic stimulation and antidepressant drug for chronic tinnitus. _Eur. Arch. Oto-Rhino-Laryngol. Off. J. Eur. Fed. Oto-Rhino-Laryngol. Soc. EUFOS Affil. Ger. Soc.
Oto-Rhino-Laryngol. - Head Neck Surg._ 272, 337–343 (2015). Google Scholar * Ting, S. K. S. _et al_. Short duration repetitive transcranial magnetic stimulation for tinnitus treatment: a
prospective Asian study. _Clin. Neurol. Neurosurg._ 113, 556–558 (2011). Article CAS PubMed Google Scholar * Anders, M. _et al_. Efficacy of repetitive transcranial magnetic stimulation
for the treatment of refractory chronic tinnitus: a randomized, placebo controlled study. _Neuro Endocrinol. Lett._ 31, 238–249 (2010). PubMed Google Scholar * Kleinjung, T. _et al_. Which
tinnitus patients benefit from transcranial magnetic stimulation? _Otolaryngol.–Head Neck Surg. Off. J. Am. Acad. Otolaryngol.-Head Neck Surg._ 137, 589–595 (2007). Article Google Scholar
* Wang, H. _et al_. A Pilot Study of EEG Source Analysis Based Repetitive Transcranial Magnetic Stimulation for the Treatment of Tinnitus. _Plos One_ 10, e0139622 (2015). Article PubMed
PubMed Central CAS Google Scholar * Langguth, B. _et al_. Transcranial Magnetic Stimulation for the Treatment of Tinnitus: A New Coil Positioning Method and First Results. _Brain Topogr._
18, 241–247 (2006). Article PubMed Google Scholar * Chung, H.-K. _et al_. Effectiveness of Theta-Burst Repetitive Transcranial Magnetic Stimulation for Treating Chronic Tinnitus.
_Audiol. Neurotol._ 17, 112–120 (2012). Article Google Scholar * Barwood, C. H. S. _et al_. The Effect of rTMS on Auditory Processing in Adults with Chronic, Bilateral Tinnitus: A
Placebo-Controlled Pilot Study. _Brain Stimulat._ 6, 752–759 (2013). Article Google Scholar * De Ridder, D., Song, J.-J. & Vanneste, S. Frontal cortex TMS for tinnitus. _Brain
Stimulat._ 6, 355–362 (2013). Article Google Scholar * Forogh, B., Yazdi-Bahri, S.-M., Ahadi, T., Fereshtehnejad, S.-M. & Raissi, G. R. Comparison of two protocols of transcranial
magnetic stimulation for treatment of chronic tinnitus: a randomized controlled clinical trial of burst repetitive versus high-frequency repetitive Transcranial Magnetic Stimulation.
_Neurol. Sci. Off. J. Ital. Neurol. Soc. Ital. Soc. Clin. Neurophysiol._ 35, 227–232 (2014). Google Scholar * Hoekstra, C. E. L., Versnel, H., Neggers, S. F. W., Niesten, M. E. F. & van
Zanten, G. A. Bilateral low-frequency repetitive transcranial magnetic stimulation of the auditory cortex in tinnitus patients is not effective: a randomised controlled trial. _Audiol.
Neurootol._ 18, 362–373 (2013). Article PubMed Google Scholar * Khedr, E. M. _et al_. Contralateral versus ipsilateral rTMS of temporoparietal cortex for the treatment of chronic
unilateral tinnitus: comparative study. _Eur. J. Neurol._ 17, 976–983 (2010). Article CAS PubMed Google Scholar * Khedr, E. M., Rothwell, J. C., Ahmed, M. A. & El-Atar, A. Effect of
daily repetitive transcranial magnetic stimulation for treatment of tinnitus: comparison of different stimulus frequencies. _J. Neurol. Neurosurg. Psychiatry_ 79, 212–215 (2008). Article
CAS PubMed Google Scholar * Kleinjung, T. _et al_. Repetitive transcranial magnetic stimulation for tinnitus treatment: no enhancement by the dopamine and noradrenaline reuptake inhibitor
bupropion. _Brain Stimulat._ 4, 65–70 (2011). Article Google Scholar * Kleinjung, T. _et al_. Levodopa does not enhance the effect of low-frequency repetitive transcranial magnetic
stimulation in tinnitus treatment. _Otolaryngol.–Head Neck Surg. Off. J. Am. Acad. Otolaryngol.-Head Neck Surg._ 140, 92–95 (2009). Article Google Scholar * Kleinjung, T. _et al_.
Long-term effects of repetitive transcranial magnetic stimulation (rTMS) in patients with chronic tinnitus. _Otolaryngol.–Head Neck Surg. Off. J. Am. Acad. Otolaryngol.-Head Neck Surg._ 132,
566–569 (2005). Article Google Scholar * Kreuzer, P. M. _et al_. A proof-of-concept study on the combination of repetitive transcranial magnetic stimulation and relaxation techniques in
chronic tinnitus. _J. Neural Transm. Vienna Austria_ 1996(123), 1147–1157 (2016). Article Google Scholar * Kreuzer, P. M. _et al_. Can Temporal Repetitive Transcranial Magnetic Stimulation
be Enhanced by Targeting Affective Components of Tinnitus with Frontal rTMS? A Randomized Controlled Pilot Trial. _Front. Syst. Neurosci._ 5, 88 (2011). Article PubMed PubMed Central
Google Scholar * Langguth, B. _et al_. High-frequency priming stimulation does not enhance the effect of low-frequency rTMS in the treatment of tinnitus. _Exp. Brain Res._ 184, 587–591
(2008). Article PubMed Google Scholar * Lehner, A., Schecklmann, M., Greenlee, M. W., Rupprecht, R. & Langguth, B. Triple-site rTMS for the treatment of chronic tinnitus: a randomized
controlled trial. _Sci. Rep._ 6, 22302 (2016). Article ADS CAS PubMed PubMed Central Google Scholar * Marcondes, R. A. _et al_. Repetitive transcranial magnetic stimulation improve
tinnitus in normal hearing patients: a double-blind controlled, clinical and neuroimaging outcome study. _Eur. J. Neurol._ 17, 38–44 (2010). Article CAS PubMed Google Scholar *
Mennemeier, M. _et al_. Variable changes in PET activity before and after rTMS treatment for tinnitus. _The Laryngoscope_ 121, 815–822 (2011). Article PubMed PubMed Central Google Scholar
* Park, S. _et al_. Combined rTMS to the auditory cortex and prefrontal cortex for tinnitus control in patients with depression: a pilot study. _Acta Otolaryngol. (Stockh.)_ 133, 600–606
(2013). Article Google Scholar * Plewnia, C. _et al_. Treatment of chronic tinnitus with theta burst stimulation: a randomized controlled trial. _Neurology_ 78, 1628–1634 (2012). Article
CAS PubMed Google Scholar * Plewnia, C. _et al_. Moderate therapeutic efficacy of positron emission tomography-navigated repetitive transcranial magnetic stimulation for chronic tinnitus:
a randomised, controlled pilot study. _J. Neurol. Neurosurg. Psychiatry_ 78, 152–156 (2007). Article CAS PubMed Google Scholar * Roland, L. T., Peelle, J. E., Kallogjeri, D., Nicklaus,
J. & Piccirillo, J. F. The effect of noninvasive brain stimulation on neural connectivity in Tinnitus: A randomized trial. _The Laryngoscope_ 126, 1201–1206 (2016). Article PubMed
Google Scholar * Sahlsten, H. _et al_. Electric field-navigated transcranial magnetic stimulation for chronic tinnitus: a randomized, placebo-controlled study. _Int. J. Audiol._ 56, 692–700
(2017). Article PubMed Google Scholar * Sahlsten, H. _et al_. Electric field navigated transcranial magnetic stimulation for chronic tinnitus: A pilot study. _Int. J. Audiol._ 54,
899–909 (2015). Article PubMed Google Scholar * Schecklmann, M. _et al_. Neuronavigated left temporal continuous theta burst stimulation in chronic tinnitus. _Restor. Neurol. Neurosci._
34, 165–175 (2016). PubMed Google Scholar * Smith, J. A. _et al_. Repetitive transcranial magnetic stimulation for tinnitus: a pilot study. _The Laryngoscope_ 117, 529–534 (2007). Article
PubMed Google Scholar * Vanneste, S. & De Ridder, D. Differences between a single session and repeated sessions of 1 Hz TMS by double-cone coil prefrontal stimulation for the
improvement of tinnitus. _Brain Stimulat._ 6, 155–159 (2013). Article Google Scholar * Yilmaz, M., Yener, M. H., Turgut, N. F., Aydin, F. & Altug, T. Effectiveness of transcranial
magnetic stimulation application in treatment of tinnitus. _J. Craniofac. Surg._ 25, 1315–1318 (2014). Article PubMed Google Scholar * Thabit, M. N., Fouad, N., Shahat, B. & Youssif,
M. Combined Central and Peripheral Stimulation for Treatment of Chronic Tinnitus: A Randomized Pilot Study. _Neurorehabil. Neural Repair_ 29, 224–233 (2015). Article PubMed Google Scholar
* Formánek, M. _et al_. Combined transcranial magnetic stimulation in the treatment of chronic tinnitus. _Ann. Clin. Transl. Neurol._ 5, 857–864 (2018). Article PubMed PubMed Central
Google Scholar Download references ACKNOWLEDGEMENTS This project was conducted as part of the European School for Interdisciplinary Tinnitus Research (ESIT) and received funding from the
European Union’s Horizon 2020 research and innovation programme under the Marie Sklodowska-Curie grant agreement number 722046. AUTHOR INFORMATION AUTHORS AND AFFILIATIONS * Department of
Psychiatry and Psychotherapy, University of Regensburg, Regensburg, Germany Stefan Schoisswohl, Jorge Simoes, Patrick Neff, Winfried Schlee, Berthold Langguth & Martin Schecklmann *
Institute of Databases and Information Systems, University of Ulm, Ulm, Germany Kushal Agrawal * University Research Priority Program “Dynamics of Healthy Aging”, University of Zurich,
Zurich, Switzerland Patrick Neff * European School for Interdisciplinary Tinnitus Research (ESIT), Regensburg, Germany Stefan Schoisswohl, Kushal Agrawal, Jorge Simoes, Winfried Schlee,
Berthold Langguth & Martin Schecklmann Authors * Stefan Schoisswohl View author publications You can also search for this author inPubMed Google Scholar * Kushal Agrawal View author
publications You can also search for this author inPubMed Google Scholar * Jorge Simoes View author publications You can also search for this author inPubMed Google Scholar * Patrick Neff
View author publications You can also search for this author inPubMed Google Scholar * Winfried Schlee View author publications You can also search for this author inPubMed Google Scholar *
Berthold Langguth View author publications You can also search for this author inPubMed Google Scholar * Martin Schecklmann View author publications You can also search for this author
inPubMed Google Scholar CONTRIBUTIONS M.S. and B.L. came up with the idea of the study. S.S. collected and analyzed the data. K.A. was involved in the literature identification process. M.S.
and S.S. wrote the main manuscript. M.S. and B.L. supervised the review. Authors W.S., J.S., P.N. and B.L. contributed to and reviewed the manuscript. CORRESPONDING AUTHOR Correspondence to
Stefan Schoisswohl. ETHICS DECLARATIONS COMPETING INTERESTS The authors declare that they have no conflict of interest associated with this publication and there has been no significant
financial or non-financial support that could have influenced its outcome. ADDITIONAL INFORMATION PUBLISHER’S NOTE: Springer Nature remains neutral with regard to jurisdictional claims in
published maps and institutional affiliations. SUPPLEMENTARY INFORMATION SUPPLEMENTAL MATERIAL 1 SUPPLEMENTAL MATERIAL 2 RIGHTS AND PERMISSIONS OPEN ACCESS This article is licensed under a
Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit
to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are
included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and
your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this
license, visit http://creativecommons.org/licenses/by/4.0/. Reprints and permissions ABOUT THIS ARTICLE CITE THIS ARTICLE Schoisswohl, S., Agrawal, K., Simoes, J. _et al._ RTMS parameters in
tinnitus trials: a systematic review. _Sci Rep_ 9, 12190 (2019). https://doi.org/10.1038/s41598-019-48750-9 Download citation * Received: 25 January 2019 * Accepted: 12 August 2019 *
Published: 21 August 2019 * DOI: https://doi.org/10.1038/s41598-019-48750-9 SHARE THIS ARTICLE Anyone you share the following link with will be able to read this content: Get shareable link
Sorry, a shareable link is not currently available for this article. Copy to clipboard Provided by the Springer Nature SharedIt content-sharing initiative